Badarpur, New Delhi – India
MUTUAL HEALTH ORGANIZATION
THE CONTEXT OF YOUR INITIATIVE
Badarpur used to be a village in older times. With the passage of time, it has developed into a squatter settlement, inhabited by large number of internal migrants. The majority of the inhabitants work in the factories as labourers/workers. Due to the closure of some industries, many of the inhabitants have lost their livelihoods and now have no stable employment. They survive by working in the unorganized sector or doing some petty jobs. Most of the women are home-based workers and are often victims of exploitation, by working for the contractors who pay them meagre wages. In recent times, due to a decline in their work orders, the women are not able to get work even from local contractors.
In view of ever increasing migration of the population from rural to urban areas, the pressure on land in the cities has increased. It has led to the establishment of urban slums (squatter settlements) in cities like Delhi. People living in these slums are living in horrible conditions, without access to basic facilities like sanitation and health. They also do not have access to the public facilities created by the Government. To make matters worse, they lack proper education/knowledge and are mostly unaware of matters concerning their health. This makes them vulnerable and exposed to malpractices and corruption of the existing healthcare providers. As a result, they end up being exploited by the doctors, hospitals and other healthcare providers and end up spending a majority of their income on health costs.
The majority of India’s population lives below the poverty line with earnings of less than 0.6 USD/day (in urban areas) and 0.4 USD (in rural areas). As the private sector dominates the healthcare sector in India, the majority living below the poverty line has to depend on the public health infrastructure. This leads to an excessive burden on the existing, insufficient public health facilities and often leads to their collapse. According to a report on healthcare in India by Price Waterhouse Coopers, India needs 74,150 community centres per million people, but it has less than half that number. Over the years, this has led to a huge gap in the existing healthcare setup and health needs of our people. During 2018-19, India spent only 1.5% of its Gross Domestic Product (GDP) on its healthcare needs, which is way below the desired goal set by the World Health Organization (WHO).
In such a scenario, where most of the private healthcare providers are driven by profits, the poor have been the worst affected. With even health insurance being out of their reach, the poor do not have any option left than to fall into the trap of healthcare providers and greedy moneylenders. This pushes them deeper into the vicious circle of poverty. People are thus being denied their right to access healthcare.
AN ALTERNATIVE – MHO
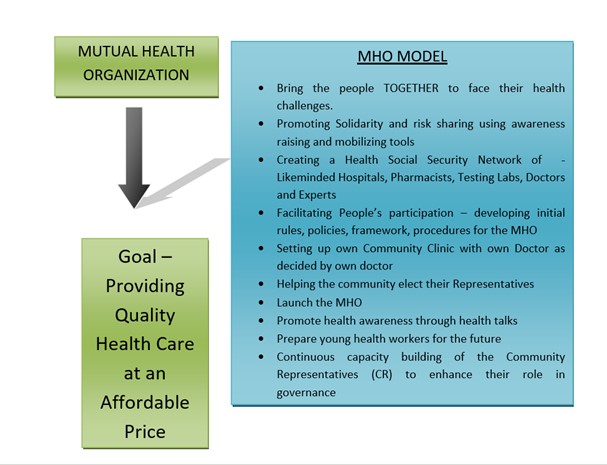
MHO offers poor people a ray of hope. MHO’s health actions, based on solidarity, self-governance and support, are the only alternatives available. MHO focuses on offering access to consultations with a general practitioner at its health centre and to medication at very low prices. It provides extensive prevention and awareness-raising work on different health aspects throughout the year within the neighbourhood, some out-patient hospital beds for observation, and partnerships developed with hospitals (public and private, of different religious denominations) in order to refer mutual health members, should this be necessary. The project is helping people to come together and support each other in their hour of need. MHO is a not-for-profit organization which offers solidarity. It is a unique initiative providing the Right to Health to those who are otherwise denied this right.
MHO provides ordinary people with some relief. By ‘Mutual’ we mean a system in which the beneficiaries themselves participate, a system which is governed by them so that they feel the responsibility of making it a success. MHO is a completely transparent system in which members with expert guidance take decisions about supporting other members. They themselves lay down the rules and follow them. MHO has, over the years, proved to be a big help in their times of need. It has taught members to behave responsibly and minimise their health costs/risks.
THE ACTIVITIES CARRIED OUT AS PART OF YOUR INITIATIVE
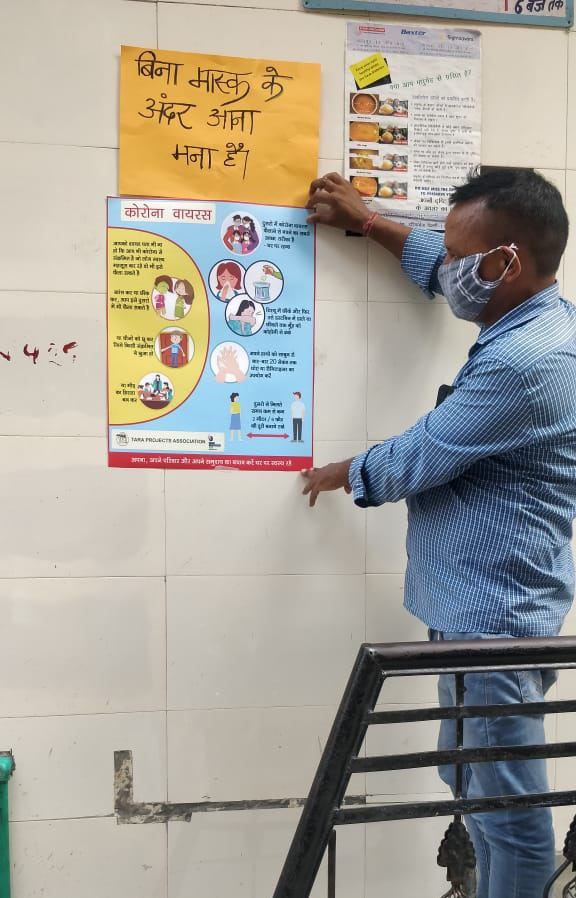
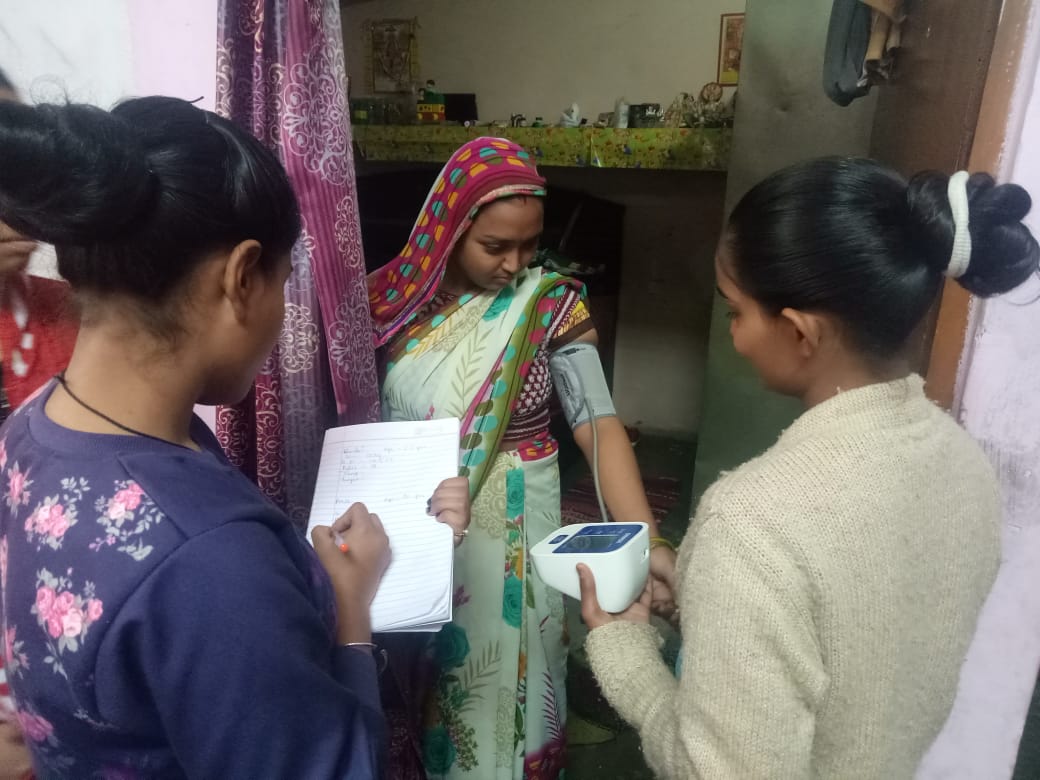
Activity 1 – Enrolment of member/family and awareness building related to preventive health care
• Awareness-raising on Mutual Healthcare and its benefits to the members on a regular basis. Home visits.
• Family includes the husband, wife, all children under 18 years of age, dependent parents, extended single family members.
• Focused group discussions with the members, enabling them to make decisions on matters such as the annual membership contribution, new facilities needed by the members, feedback about the existing services. So far, the members have decided that the annual contribution should be 2.70 USD per person for a family of 4 and above. For a family with fewer than 4 members, the annual contribution has been set at 3.38 USD per member.
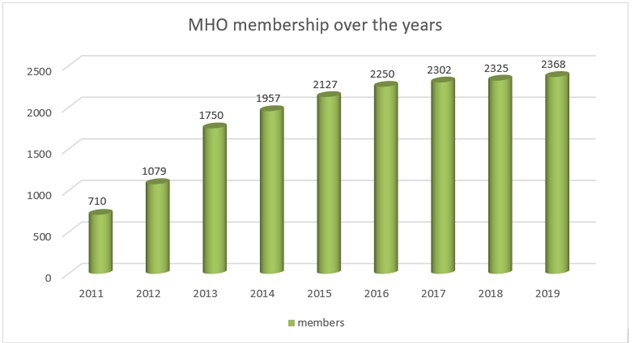
• More than 2,368 members have joined MHO to date.
Activity 2 – Governance
• MHO members are responsible for the identification and nomination of community representatives (CR), who are the face of the larger group. Six community representatives have been elected by the members.
• Training of the community representatives on the MHO, its rules, financial management, decision making, Emmaus values and public speaking.
• MHO has a separate bank account for the member’s contributions. This account is operated by two of the elected community representatives, along with one signatory from Tara.
• Holding an Annual General Assembly of MHO including all the members.
• Identification, collaboration and networking with the nearby nursing homes, public and private hospitals, laboratories and pharmacists. Agreement with the health care providers for discounted treatment/tests.
Activity 3 – Setting up a Health Clinic
• A primary healthcare centre/clinic has been set up with a doctor and one paramedic to provide treatment and medicines. So far more than 57,000 patients, both members and non-members, have been given medical consultations and medicines.
• The members have jointly decided on a nominal fee for persons visiting the MHO health clinic. It helps recover the cost of medicines.
• Maintaining a record of membership including the member’s family details.
• The membership is for one year and can be renewed annually.
• Organising regular health talks and medical health camps in collaboration with hospitals and trained healthcare personnel. More than 350 health talks have been organised so far. During the health camps, MHO organises for specialists to come for a day, providing more specific care, with free access for all members to ophthalmic or gynaecological care, for example. MHO covers the costs of these visits.
Activity 4 – Reimbursement of Hospitalisation Claims (cost incurred by members if hospitalised)
• Cost of hospitalisation claims (submitted by the members).
• Each claim is discussed by the Community Representatives (CR) in a claims meeting, along with the Tara Representatives.
• Decisions regarding the reimbursement of the claim are taken by the local MHO Committee of Community Representatives, based on invoices received and the MHO Policy Document (developed by the CR).
• The records of these meetings are properly documented and filed by MHO.
• More than 80 member beneficiaries have been granted their hospitalisation claims by MHO.
In total, more than 75,000 medical treatments (consultations at the centre, referrals to hospitals or laboratories, hospital stays, etc.) have been provided since the inception of the project in 2011.
Facilities Offered by MHO
MHO has created a self-support system built around its members. The members are entitled to the following facilities as per MHO rules:
• Access to medical treatment at a low fee of only 0.27 USD (while on the open market, the lowest consultation fee is 1.35 USD).
• Reimbursement of costs incurred by a member for hospitalisation.
• 50% discount on medical tests.
• Preventive health talks to create awareness about responsible health behaviour.
• Health Camps and the provision of free medicines to members.
• Physiotherapy facility.
• Eye and dental care facility with free eye surgery through our network.
• Network of private and public hospitals to support the members (we encourage use of public hospitals).
• Participatory approach and mutual decision making.
• The members are key stakeholders in the whole MHO eco-system.
WHO IS INVOLVED FROM OUR GROUP?
8 staff members, 6 community representatives, 6 volunteers, are involved in the project.
WHICH PARTNERS ARE YOU WORKING WITH ON THIS INITIATIVE?
Photos













FUTURE PROSPECTS
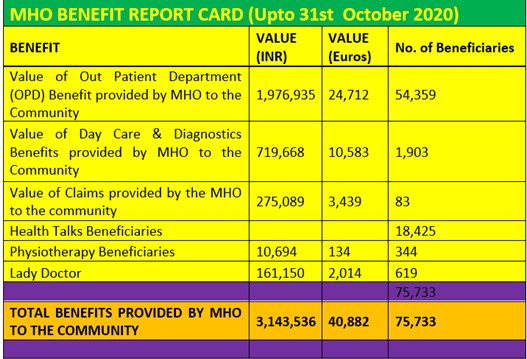
See table “MHO benefit report card”
WOULD YOU LIKE TO ADD ANY INFORMATION ABOUT YOUR INITIATIVE?
WHAT ARE YOUR PROSPECTS?
Sustainability Plan
• To cover more members to MHO. The long term plan is to reach 15,000 beneficiaries.
• Utilisation of corpus/membership fee to cover some costs of MHO.
• Increase the revenue of the MHO Clinic and utilise the same to cover some costs of the project.
• Training of youths to take responsibility as community representatives.
• Focus more on improving overall hygiene of the member families to reduce the number of people falling sick.
• Promote MHO among other support organizations for getting external support.
• Expanding MHO actions to other areas.
• Extend MHO to Family Health Sponsorship plan.
On the same topic

ARTS AND VOCATIONAL TRAINING SCHOOL
Pereira, Risaralda – Colombia
Rehabilitation through the Carnival in Prisons for Women
Montevideo – Uruguay
PASSIONE CIVILE
Palerme – ItalyLatest news